Berberine for Candida Overgrowth: Multi-Target Antifungal Mechanisms
Research review on berberine's biofilm disruption and systemic effects against Candida

This perspective is authored by a credentialed provider practicing outside their primary specialty. Readers should weigh this context.
Background
Candida overgrowth represents a complex clinical challenge that extends far beyond typical superficial yeast infections. While commonly associated with oral thrush and vaginal infections, pathogenic Candida species demonstrate sophisticated survival mechanisms including biofilm formation, morphological transformation, and immune system evasion that can lead to systemic manifestations.
Traditional antifungal approaches often fail to address the full spectrum of Candida's pathogenic capabilities. The organism's ability to form protective biofilms, shift between yeast and hyphal forms, and develop drug resistance through efflux pump mechanisms creates treatment-resistant infections. Furthermore, Candida can engage in molecular mimicry, confusing immune system recognition and contributing to symptoms ranging from brain fog to gastrointestinal dysfunction.

The clinical significance extends to metabolic health, as Candida overgrowth often coincides with dysregulated glucose metabolism, creating a self-perpetuating cycle where elevated blood sugar feeds fungal growth. This relationship has prompted investigation into compounds that can simultaneously address antifungal activity and metabolic regulation, with berberine emerging as a promising multi-target therapeutic approach.
Key Findings
Biofilm Disruption and Direct Antifungal Activity
Laboratory studies demonstrate berberine achieves up to 96.93% biofilm inhibition in C. krusei after 48 hours of treatment[1][4][5][6][7][8][9], with minimal resistance development observed. This represents a significant advancement over conventional antifungals that struggle with established biofilms.
Novel Mechanism of Action
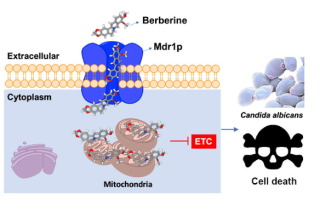
Berberine demonstrates a unique mechanism by hijacking Candida's own efflux pumps—the same systems responsible for drug resistance. Rather than being expelled, berberine exploits these pumps as entry points, creating a "Trojan horse" effect that bypasses traditional resistance mechanisms.
Multi-Target Cellular Effects
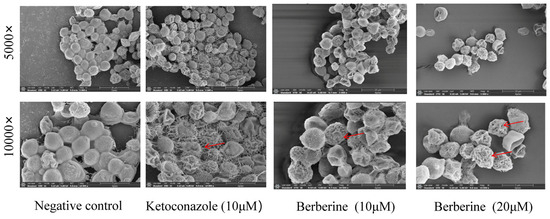
Once intracellular, berberine coordinates a seven-pronged assault on fungal viability. A 2024 study found berberine binds to CYP51, the enzyme responsible for ergosterol synthesis—Candida's equivalent of cholesterol. Simultaneously, berberine strips up to 77.11% of membrane sterols, causing structural collapse of the fungal cell wall[2][3].

At concentrations of 17.75 μg/ml, berberine completely prevents germ tube formation by suppressing both cAMP-PKA and MAPK pathways. This effectively blocks Candida's transformation into its invasive hyphal form, preventing tissue penetration and translocation.
Selective Antimicrobial Activity
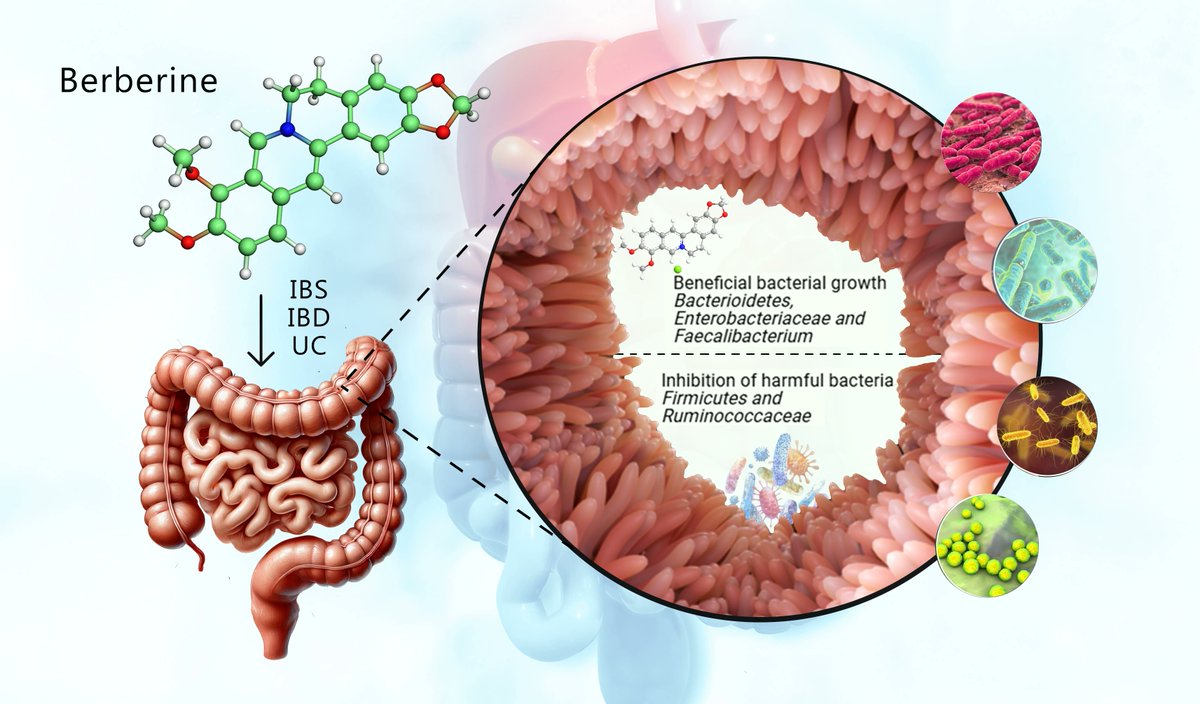
While demonstrating potent antifungal effects at concentrations of 17.75 to 80 μg/ml, berberine shows remarkable selectivity for pathogenic organisms. Beneficial bacterial populations actually increase, with Bifidobacterium populations rising by 60% and Akkermansia muciniphila flourishing under berberine treatment.
Metabolic Integration
Berberine's systemic effects extend beyond direct antifungal activity to address the metabolic environment that supports Candida growth. Studies show significant improvements in glucose regulation within weeks of treatment initiation, creating an inhospitable environment for fungal proliferation while supporting overall metabolic health.
Methodology Notes
The evidence base for berberine's anti-Candida effects primarily derives from in vitro laboratory studies and mechanistic research rather than large-scale clinical trials. While these studies provide valuable insights into berberine's mechanisms of action, translation to clinical outcomes requires careful consideration of study limitations.
Most biofilm inhibition and morphological transformation data comes from controlled laboratory conditions using standardized Candida strains. Real-world fungal infections involve complex polymicrobial environments and patient-specific factors that may influence treatment response. The 96.93% biofilm inhibition rate, while impressive in laboratory settings, may not directly translate to clinical efficacy rates.
Concentration-dependent effects noted in studies (17.75-80 μg/ml for antifungal activity) require pharmacokinetic validation to ensure achievable tissue levels in clinical use. The selectivity for pathogenic vs. beneficial organisms, while promising, needs confirmation in human microbiome studies rather than isolated bacterial culture systems.
The metabolic effects of berberine on glucose regulation are better supported by clinical trial data, though most studies focus on diabetes management rather than anti-Candida outcomes. The connection between improved glucose control and reduced fungal growth, while mechanistically sound, represents an extrapolation from separate research domains.
Clinical Relevance
Berberine's multi-target approach addresses several clinical challenges in Candida management that conventional antifungals fail to resolve. The ability to disrupt established biofilms while preventing morphological transformation represents a significant advancement for patients with recurrent or treatment-resistant fungal overgrowth.
The compound's selectivity for pathogenic organisms while promoting beneficial bacteria offers a distinct advantage over broad-spectrum antifungals that often worsen dysbiosis. This characteristic is particularly relevant for patients with concurrent gastrointestinal symptoms or those requiring long-term antifungal therapy.
From a practical standpoint, berberine's established safety profile and availability as a dietary supplement makes it accessible for clinical use, though standardization and dosing protocols require development. The suggested synergistic combinations with MCT oil (3 teaspoons daily) and lactoferrin (400mg) provide a framework for comprehensive treatment protocols.

However, clinicians should be prepared for Herxheimer reactions, which typically occur within 24-72 hours of treatment initiation. These die-off reactions can temporarily worsen symptoms and require appropriate patient counseling and supportive management. The metabolic benefits may provide additional value for patients with concurrent insulin resistance or metabolic syndrome.
The integration of blood sugar management through myoinositol supplementation (2g twice daily) and dietary modifications (limiting carbohydrates to 40-50g per meal) reflects a systems-based approach that addresses root causes rather than just symptoms.
Future Directions
Clinical trials are needed to validate berberine's in vitro anti-Candida effects in human subjects. Randomized controlled trials comparing berberine-based protocols to standard antifungal therapy would provide crucial efficacy and safety data for evidence-based recommendations.
Pharmacokinetic studies should establish optimal dosing regimens to achieve therapeutic tissue concentrations while minimizing adverse effects. Research into bioavailability enhancement and targeted delivery systems could improve clinical outcomes and reduce dosing requirements.
The synergistic effects of combination protocols (berberine plus MCT oil, lactoferrin, and metabolic support) require systematic evaluation to determine optimal ratios and timing. Understanding which patients benefit most from multi-component approaches versus berberine monotherapy would inform personalized treatment strategies.

Long-term safety studies are essential, particularly for patients requiring extended treatment courses. Investigation into resistance development patterns and strategies to prevent them will inform sustainable treatment protocols. Additionally, research into biomarkers for treatment response could improve monitoring and optimize treatment duration.
Frequently Asked Questions
What makes berberine different from conventional antifungal medications?
What is the typical dosage and duration for berberine in Candida treatment?
What is a Herxheimer reaction and how should it be managed?
Can berberine be combined with other antifungal treatments?
How does berberine affect blood sugar and why is this important for Candida treatment?
References
- [1]Xie Y, Liu X, Zhou P. In vitro Antifungal Effects of Berberine Againstspp. In Planktonic and Biofilm Conditions. Drug Des Devel Ther. 2020. [PMID: 32021094 | doi:10.2147/DDDT.S230857]
- [2]Ding J, Yan Z, Peng L, et al. Inhibitory effects of berberine on fungal growth, biofilm formation, virulence, and drug resistance as an antifungal drug and adjuvant with prospects for future applications. World J Microbiol Biotechnol. 2024. [PMID: 39690297 | doi:10.1007/s11274-024-04223-4]
- [3]Li Y, Liu Y, Jiang Y, et al. New antifungal strategies and drug development against WHO critical priority fungal pathogens. Front Cell Infect Microbiol. 2025. [PMID: 41078362 | doi:10.3389/fcimb.2025.1662442]
- [4]da Silva JSSC, Barbaresco MJ, Rocha RM, et al. Chlorhexidine combined with curcumin-mediated photodynamic treatment effectively inhibits biofilm formation by clinical Candida isolates from the oral cavity. Photodiagnosis Photodyn Ther. 2025. [PMID: 40651738 | doi:10.1016/j.pdpdt.2025.104709]
- [5]Alawadi A, AbdulAzees PA, Lin CY, et al. Application of organoselenium in inhibiting Candida albicans biofilm adhesion on 3D printed denture base material. J Prosthodont. 2024. [PMID: 37422719 | doi:10.1111/jopr.13733]
- [6]A. K. Chan, Y. C. Tsang, C. Chu, et al. Aspirin as an Antifungal-Lock Agent in Inhibition of Candidal Biofilm Formation in Surgical Catheters. Infection and Drug Resistance. 2021. [PMID: 33888996 | doi:10.2147/IDR.S308262]
- [7]V. Balázs, Lili Puskár, E. Ormai, et al. Synergistic Anti-Candida Effects of Essential Oil Blends on Biofilms at Various Maturation Stages. European journal of pharmaceutical sciences : official journal of the European Federation for Pharmaceutical Sciences. 2026. [PMID: 41871816 | doi:10.1016/j.ejps.2026.107515]
- [8]Neda AlMojel, Parveez Ahamed AbdulAzees, E. Lamb, et al. Determining growth inhibition of Candida albicans biofilm on denture materials after application of an organoselenium-containing dental sealant. The Journal of prosthetic dentistry. 2021. [PMID: 34078547 | doi:10.1016/j.prosdent.2021.04.015]
- [9]Ciurea CN, Mare AD, Mareş M, et al. The influence of farnesol and tyrosol onspp. virulence traits. Germs. 2024. [PMID: 40271088 | doi:10.18683/germs.2024.1444]
This information is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider regarding any medical condition or treatment plan.
This content represents one clinician’s clinical perspective and approach.
Published:
Last updated: